UPDATE: In June 2014, Ning Liang, one of the founders of HealthSherpa, wrote in about updates to the site. Ling said that they can now enroll people in ACA marketplace plans, including subsidies. According to Liang, “we are the only place besides Healthcare.gov where this is possible. We have signed an agreement with CMS as a web based entity to do this. We are directly integrated with the federal data hub, so going through us is identical to going through Healthcare.gov.”
Earlier tonight, Levick director of digital content Simon Owens discovered HealthSherpa.com, thought it was cool, and read a Daily Dot post about it that framed it as 3 20-something San Francisco Bay-area resident coding up an alternative to Healthcare.gov.
Could it be that easy, wondered Owens? Could these young coders have created a simpler, better way to shop for health insurance than the troubled Healthcare.gov?
Well, yes and no. As is so often the case, it’s not quite that simple, for several reasons.
1) As always, note the disclaimer at the bottom of HealthSherpa.com: “The information provided here is for research purposes. Make sure to verify premiums and subsidies on your state exchange or healthcare.gov, or directly with the insurance company or an agent.”
Why? The site is based upon the publicly available data published by the Department for Health and Human Services, individual state exchanges and Healthcare.gov for premium costs, like this dataset of premiums by county at data.healthcare.gov.
Unfortunately, there appear to be data quality issues, as CBS News reported, that may be an issue on both sites.
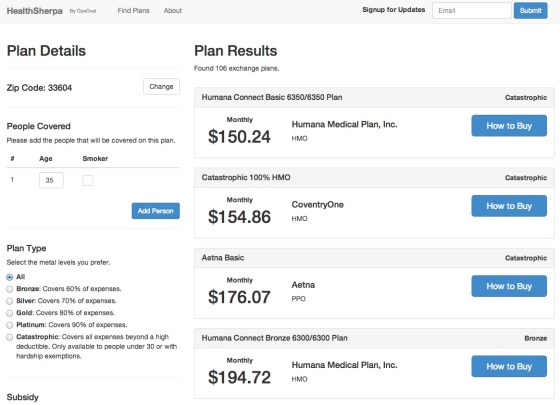
When I compared searches for the same zipcode in Florida for a 35 year old, single non-smoking male, I found the same 106 plans but was quoted different premiums: $128.85 on HC.gov vs $150.24 on HealthSherpa. Hmm.
That could be user error, but… it looks like Healthcare.gov continues to underestimate costs.
Healthsherpa may actually be doing better, here. Good job, guys.
2) Regardless, this is not a replacement for everything Healthcare.gov is supposed to do.
The federal and state exchanges aren’t just about browsing plans and comparing premiums for options in a given zipcode in the “marketplace.” After a user knows decides which plan he or she want, the software is supposed to:
1) Register them as a user (registration was up front initially, which was a controversial, important choice, relevant to the site crashing at launch)
2) Authenticate them against government data bases
3) Verify income against government data bases
4) Calculate relevant subsidies, based upon income
5) Guide them through the application process
6) Send that form data on to insurance companies for enrollment.
The tech that underpins the test and graphics website on the front end of those process continues to hold up well.
The rest of the software that is supposed to enable visitors to go through steps 1-6 software, not so much. 16 state exchanges and DC are having varying degrees of success, with HHS Secretary Kathleen Sebelius acknowledging issues with data quality in Step 6 in her testimony to Congress.
3) While it has a subsidy calculator, otherwise Healthsherpa doesn’t replace Healthcare.gov.
Healthsherpa enables you to find a relevant plan and then gives you contact info for the relevant insurer.
For instance:
“Call Humana Medical Plan, Inc. at (800) 448-6262.
Use their menu or ask the operator to speak to someone about purchasing coverage.
Tell them you would like to purchase health exchange coverage, specifically the Humana Connect Basic 6350/6350 Plan for Hillsborough County, FL.
Follow their instructions to complete the application process.”
It does not place calls to the data hub to calculate steps 1-6.
That limited functionality, however, has been good enough for U.S. Senator Angus King to recommend HealthSherpa as a temporary alternative to Healthcare.gov.
“HealthSherpa offers a user-friendly platform to quickly browse through available health insurance plan options, including monthly premium costs, coverage plans, and possible premium subsidies,” Senator King said. “I recommend that Mainers who are having trouble with Healthcare.gov use HealthSherpa as a temporary alternative until the federal website functions properly.”
4) There are OTHER private healthcare insurance brokers that could be doing this.
Back in May 2013, the Center for Medicare and Medicaid Services issued official guidance for private sector brokers in online health insurance marketplaces. (PDF)
Former U.S. chief technology officer Aneesh Chopra said that these “Web-based entities” will be online this fall, operated by entities like eHealthInsurance.com and GetInsured.
For some reason, however, private sector insurance brokers have been stymied by the federal government from selling ACA insurance policies.
That’s unfortunate, given that the Obama administration could use a Plan B, just in case the progress on Healthcare.gov doesn’t lead to a functional federal health insurance exchange twenty days from now.
Update: Jonathan Cohn, writing for the New Republic, looked into Healthcare.gov’s backup plan and comes up with an interesting detail: issues with the so-called data hub could be holding back deployment of private online health insurance brokers.
…administration officials have been huddling with insurers about how to make more use of direct enrollment. Step one is to make sure that “side door” enrollment works smoothly. It doesn’t function well right now, because—you guessed it—it relies on the same information technology system that powers healthcare.gov. Fixing that portal, which techies tell me is called an “application programming interface,” is high on the administration’s to-do list. But it’s not clear (to me) whether improving the portal might require design modifications—or to what extent its success depends upon other, ongoing repairs to the federal website.
So, here’s some speculation: While it’s hard to know for sure, but it’s quite likely that that “portal” is the data hub that’s behind Healthcare.gov, and that it may not be up to additional volume from private sector demand.
The federal exchange and state exchanges both rely upon it, and, while federal officials have said that it’s working, a report by the New York Times yesterday that some state health insurance exchange are continuing to battle tech problems indicated that it’s not holding up under demand:
Even states whose websites are working well say they are hampered by a common problem: the federal website, particularly the data hub that checks every applicant’s identity and eligibility. That hub has stopped working on several occasions, preventing applications in the states from being completed.
If that’s happening now, concerns about the ability of the hub to hold up under the pressure of private sector online insurance brokers could well be justified. If I learn anything more definitive, I’ll share it.